- What is Erectile Dysfunction and Its Link to Diabetes
- Type 1 vs. Type 2 Diabetes and Erectile Dysfunction
- Why Diabetes Causes Erectile Dysfunction?
- Factors that Increase Erectile Dysfunction Risk in Diabetic Patients
- Diabetes and Erectile Dysfunction Pathophysiology
- Treatment Options for Diabetes-Related Erectile Dysfunction
- Penile Implant for Diabetes-Associated Erectile Dysfunction
- Does Diabetes Management Treat Erectile Dysfunction?
- Erectile Dysfunction as an Early Indicator of Diabetes (Pre-Diabetes)
- Lifestyle, Medication, and Management Tips
- Coding Diabetes and Erectile Dysfunction
- Takeaways about Diabetes and Erectile Dysfunction
- Regain Sexual Confidence with a Penile Implant
- FAQs About Diabetes and Erectile Dysfunction
Men with diabetes mellitus (DM), whether type 1 or type 2, are up to 3.5 times more likely to experience erectile dysfunction (ED). Chronic high blood sugar can damage nerves and blood vessels, reduce circulation, and cause hormonal imbalances, all contributing to sexual difficulties. Early detection and proper glucose control can prevent further damage and reduce the risk of ED. While common, ED is often treatable through lifestyle changes, medication, and medical interventions.
Don’t waitconsult a specialist today to explore effective treatment options and take back control of your sexual health.
What is Erectile Dysfunction and Its Link to Diabetes

Erectile dysfunction (ED), formerly known as impotence, is the consistent inability to achieve or maintain a penile erection sufficient for satisfactory sexual performance.
Approximately 50% of men with diabetes experience ED, and prediabetic patients can also be affected. Pre-diabetes is strongly associated with a higher prevalence of erectile dysfunction, highlighting the importance of early metabolic control.
The chronic hyperglycemia that is associated with Diabetes mellitus (DM) contributes to ED pathophysiology by damaging nerves and blood vessels, reducing penile blood flow, decreasing nitric oxide levels, and increasing oxidative stress. These changes often cause ED to occur at younger ages compared to men without diabetes.
Type 1 vs. Type 2 Diabetes and Erectile Dysfunction
ED is more common in type 2 diabetes, affecting roughly 66.3% of patients, compared to about 37.5% in type 1 diabetes. It often appears 10–15 years earlier in diabetic men, with a risk approximately 3.5 times higher than in non-diabetic men, and the risk increases further with poorly controlled blood sugar.
Why Diabetes Causes Erectile Dysfunction?

Diabetes significantly impacts sexual function by damaging the nerves and blood vessels essential for an erection. Hormonal imbalances and reduced circulation can further compromise erectile ability. Studies show that ED is much more common in men with diabetes than in the general population, underscoring the importance of early monitoring and intervention.
1. Hyperglycemia
Chronic high blood glucose in diabetes damages nerves (neuropathy) and penile blood vessels, impairing blood flow required for erections. Key mechanisms include:
- Oxidative stress and endothelial dysfunction, reducing nitric oxide (NO) and smooth muscle relaxation
- Advanced glycation end-products (AGEs), causing structural tissue damage
- Neural impairment affecting both sensory and autonomic nerves
These changes result in reduced penile blood flow, impaired cavernosal smooth muscle function, and structural alterations in erectile tissue, contributing to diabetes-induced erectile dysfunction.
Results of damaging penile blood flow are:
- Blood flow to the penis decreases
- Cavernosal smooth muscle relaxation becomes impaired
- Erectile tissue may undergo structural changes
2. Comorbidities
Other conditions commonly associated with diabetes can worsen ED:
- Hypertension: Arterial stiffness, reduced NO, impaired penile blood flow
- Dyslipidemia: Accelerates atherosclerosis, reducing penile circulation
- Obesity & Metabolic Syndrome (MetS): Cause chronic inflammation, insulin resistance, and endothelial dysfunction
- Hypogonadism (Low Testosterone): Reduces erectile function, libido, and vascular health
3. Age Factor
While aging increases ED risk for all men, diabetic men often experience erectile problems earlier, sometimes even before diabetes or cardiovascular disease is diagnosed.
Factors that Increase Erectile Dysfunction Risk in Diabetic Patients
- Longer diabetes duration: More time with diabetes causes cumulative nerve and blood vessel damage.
- Poor blood sugar control: High glucose accelerates vascular and nerve injury.
- Advanced age: Aging reduces blood flow and nerve function, worsened by diabetes.
- Diabetes-related complications: Conditions like neuropathy and cardiovascular disease further impair erectile function
These factors contribute to progressive vascular and neurological damage, which are essential for normal erectile function.
Diabetes and Erectile Dysfunction Pathophysiology
Diabetes-induced erectile dysfunction (DIED) is a multifaceted and often early-onset complication driven by chronic hyperglycemia, which damages nerves and blood vessels essential for erections. The underlying pathophysiology of diabetes and erectile dysfunction involves:
- Oxidative stress and reactive oxygen species (ROS) that impair arterial inflow to the corpus cavernosum
- Endothelial dysfunction, leading to decreased nitric oxide (NO) bioavailability and reduced smooth muscle relaxation
- Advanced glycation end-products (AGEs), causing structural damage to penile tissue
- Neural damage affecting both sensory and autonomic nerves essential for normal erectile function
- Hypogonadism (low testosterone), which further impairs libido, vascular health, and erectile ability
Treatment Options for Diabetes-Related Erectile Dysfunction
Treating erectile dysfunction (ED) in men with diabetes requires a comprehensive approach, primarily focusing on strict blood sugar control, lifestyle modifications (weight loss, regular exercise, and smoking cessation), and the first-line use of PDE5 inhibitors such as Viagra or Cialis. If these treatments are not effective, other options include intracavernosal injections, vacuum erection devices, or penile implants.
While there is no absolute “cure” that can fully reverse the nerve or vascular damage caused by diabetes, erectile dysfunction in diabetic men is highly treatable and often manageable through improved glycemic control combined with targeted ED treatments.
Treatment options for ED in diabetic men are diverse, and the choice depends on:
- Severity of ED
- Desired durability of results
- Cost considerations
- Invasiveness of the procedure
Treatment is not dependent on the type of diabetes. Options range from oral medications (such as PDE5 inhibitors) to injectable therapies, vacuum devices, and penile implants. With the right treatment, many men can restore erectile function, regain confidence, and improve their overall quality of life.
Medications and treatments options for ED in diabetic patients
Treating erectile dysfunction (ED) in men with diabetes requires a multi-layered approach, often combining pharmacological treatments, devices, surgical options, and lifestyle optimization.
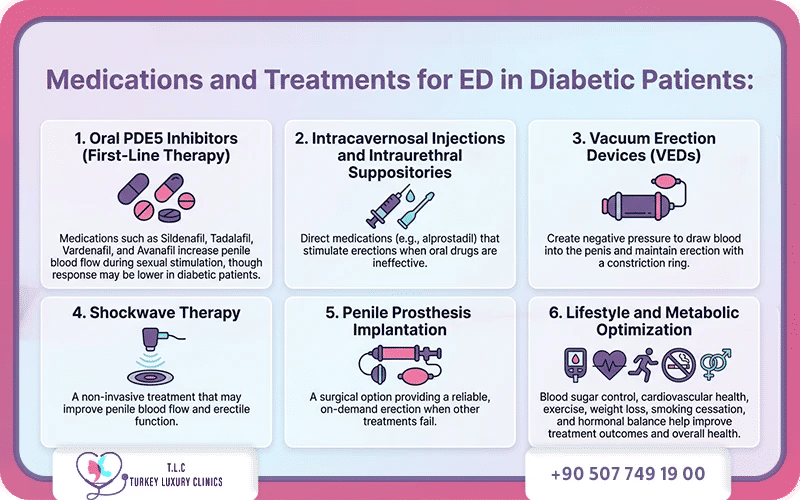
1. Oral PDE5 Inhibitors (First-Line Therapy)
Phosphodiesterase type-5 (PDE5) inhibitors are the primary treatment for ED in diabetic men. Common medications include:
- Sildenafil
- Tadalafil
- Vardenafil
- Avanafil
These drugs enhance nitric oxide–mediated vasodilation, increasing blood flow to the penis during sexual stimulation. Response rates may be lower in diabetic patients due to nerve and vascular damage.
2. Intracavernosal Injections and Intraurethral Suppositories
For men who do not respond to oral medications:
- Intracavernosal injections (e.g., alprostadil, or combinations with papaverine and phentolamine) directly stimulate penile tissue to produce an erection.
- Intraurethral suppositories deliver medication into the urethra for local effect.
These methods bypass vascular limitations and are highly effective when oral drugs fail.
3. Vacuum Erection Devices (VEDs)
Vacuum devices create negative pressure around the penis, drawing blood into the erectile tissue and producing an erection. A constriction ring maintains rigidity.
- Suitable for men seeking non-drug, non-invasive options
- Can be used alone or with medications
- Erections may feel less natural than spontaneous erections
4. Shockwave Therapy
An emerging, non-invasive treatment that targets the underlying vascular causes of ED. Early studies suggest it may improve penile blood flow and erectile function, though more research is ongoing.
5. Penile Prosthesis Implantation
For severe or refractory ED, surgical implantation of a penile prosthesis provides a permanent, reliable solution. Men can achieve an erection on demand, even when other therapies have failed.
6. Lifestyle and Metabolic Optimization
Optimizing overall health enhances ED treatment effectiveness:
- Blood sugar control
- Cardiovascular health management
- Regular exercise and weight loss
- Smoking cessation
- Hormonal correction (e.g., testosterone replacement if needed)
These measures not only support erectile function but also improve overall well-being and quality of life.
Penile Implant for Diabetes-Associated Erectile Dysfunction
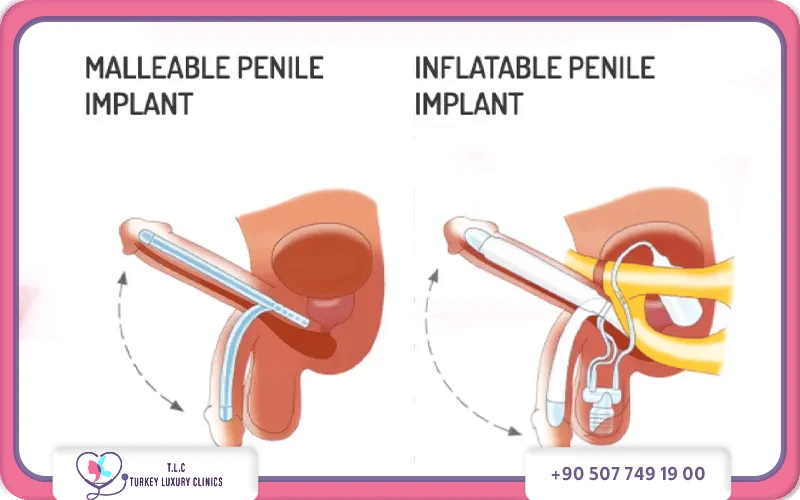
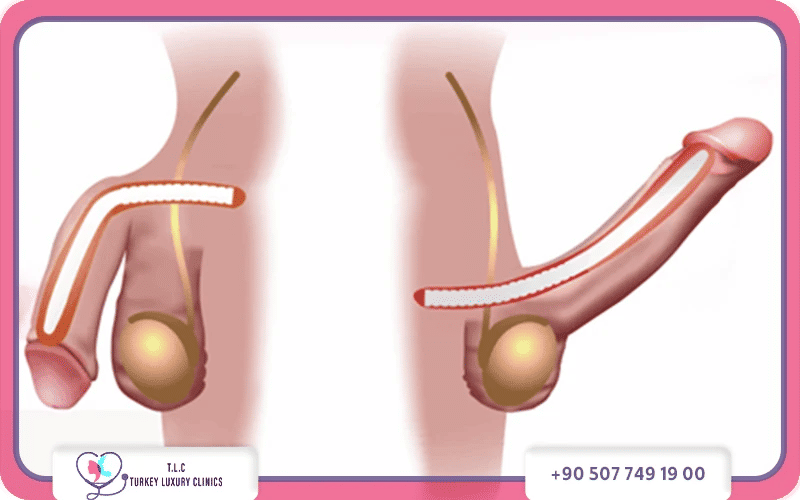
Penile implants (PPI) are a highly effective and definitive treatment for men with diabetes (DM) who have severe, irreversible erectile dysfunction, with patient satisfaction rates of 80–90%. Both inflatable and malleable devices are used to restore erectile function.
While the risk of infection is slightly higher in diabetic patients (about 3% vs. 2% in non-diabetics), implants remain a safe and reliable option when glycemic control is maintained (HbA1c <8–9%).
Penile implants are typically considered when ED medications fail to provide satisfactory erections or their effectiveness decreases over time.
Because diabetes often causes vascular and neurological impairment, oral medications such as sildenafil (Viagra) may be ineffective, making penile implants the superior solution for restoring potency.
Inflatable penile prostheses (IPPs), in particular, have shown high effectiveness and patient satisfaction in managing DM-associated ED, despite diabetics having an approximately two-fold higher risk of infection compared to non-diabetics.
Does Diabetes Management Treat Erectile Dysfunction?
Early glycemic control may reduce progression to diabetes and mitigate vascular and neurological complications that contribute to ED.
Proper diabetes control, through blood sugar monitoring (fasting glucose tests) and HbA1c management, is crucial to prevent further nerve and vascular damage. While glucose management cannot reverse damage that has already occurred, it is an essential first step. Treating ED without controlling blood sugar is often ineffective, and the condition may worsen over time.
In practice, a combined approach—managing diabetes while using targeted ED treatments—offers the best chance for safe, lasting, and effective results.
Importance of Early DM Diagnosis for ED prevention:
Early identification of metabolic abnormalities in men presenting with ED is clinically important because:
- It allows early intervention for diabetes or prediabetes
- Lifestyle modifications may prevent progression to type 2 diabetes
- Improved metabolic control may help improve erectile function
Lifestyle strategies such as dietary modification, weight management, and regular physical activity are often recommended as part of the treatment approach.
Erectile Dysfunction as an Early Indicator of Diabetes (Pre-Diabetes)
Erectile dysfunction can sometimes be an early clinical manifestation of undiagnosed diabetes. Clinical observations suggest that approximately 1 in 5 men who seek medical evaluation for erectile dysfunction are subsequently diagnosed with diabetes mellitus.
Young men who experience ED need to be evaluated for DM through these tests:
- HbA1c (glycated hemoglobin)
- Serum insulin levels
- Postprandial blood glucose measurements
Because penile arteries are relatively small, vascular impairment caused by metabolic disorders may appear in erectile function before other cardiovascular symptoms become evident.
Lifestyle, Medication, and Management Tips

- Optimize glycemic control to prevent or limit neuropathy and vascular damage.
- Smoking cessation and alcohol moderation.
- Regular physical activity and weight management.
- Heart-healthy diet to support vascular function.
Coding Diabetes and Erectile Dysfunction
Coding for diabetes-related erectile dysfunction (ED) typically involves using ICD-10 code N52.1 (Erectile dysfunction due to diseases classified elsewhere) as the primary diagnosis, along with the specific diabetes code:
- E11.9 – Type 2 diabetes mellitus without complications
- E10.9 – Type 1 diabetes mellitus without complications
This coding approach reflects that ED in diabetic patients is often a vascular or neural complication of the underlying disease. Read about ICD10 for Penile Prosthesis
Takeaways about Diabetes and Erectile Dysfunction
- Diabetes significantly increases the risk of ED, with around 50% of men with diabetes experiencing it.
- Chronic hyperglycemia damages penile blood vessels and erectile tissue, contributing to ED.
- Erectile dysfunction may serve as an early marker of prediabetic metabolic disease.
- Full metabolic screening is recommended for men presenting with ED.
- Early diagnosis and metabolic control can improve both general health and sexual function.
- First-line therapy involves PDE5 inhibitors, while second-line options include intracavernosal injections (alprostadil alone or in combination with papaverine and phentolamine).
- Penile prosthesis implantation is a definitive solution and the most effective option when conservative and medical therapies fail.
Regain Sexual Confidence with a Penile Implant
Struggling with diabetes-related ED? A penile implant could restore your sexual confidence. Consult a urologist today. Contact us at Turkey Luxury Clinics for free consultation.